Health & Fitness
Where Does it Hurt? Spondylolysis
Low back pain caused by sport induced repetitive fracture or Spondylolysis is not uncommon. Learn the warning signs and how to reduce your risk in this months Where Does it Hurt?
Over the last few years we have seen a fair number of low back complaints which were spodylolytic in origin. I would first like to clarify with some definitions of two other similar terms which are often times confused. Spondylosis, spondylolisthesis, and spondylolysis are a mouthful so lets set the record straight.
Spondylosis - A degeneration of the spinal articulations. Essentially the same as arthritis of the spine. Also called spinal osteoarthritis.
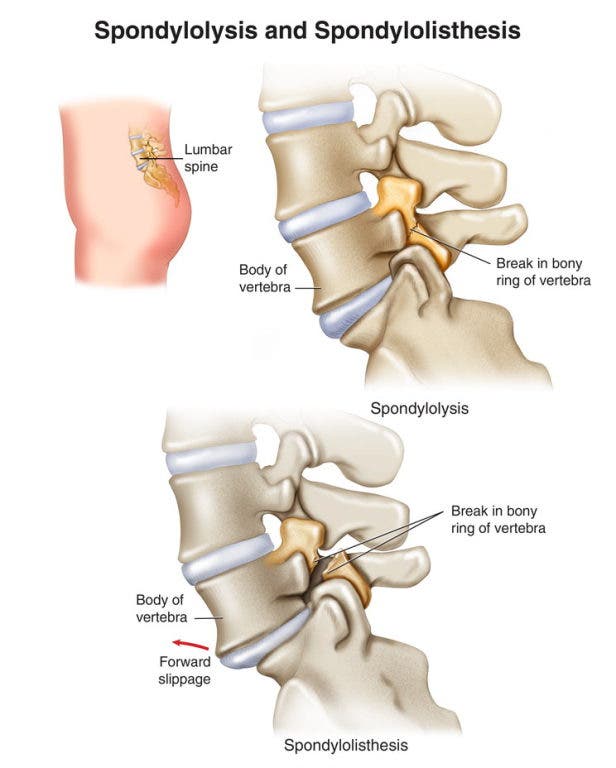
Spondylolisthesis - An anterior or posterior displacement of a vertebral segment in relation to the bone above or below.
Find out what's happening in Smithtownwith free, real-time updates from Patch.
Spondylolysis - A defect in a lumbar vertebra - an interruption in the continuity of the bone at the pars interarticularis. In other words: a break in the bone.
Statistics:
Find out what's happening in Smithtownwith free, real-time updates from Patch.
- Spondylolysis occurs in 6% of the general population, and 8-14% of elite adolescent athletes.
- Boys have a higher incidence than girls.
- Incidence in young female gymnasts is 4X greater than the general female population.
- 85% of Spondylolysis’ are reported in the L5 vertebra.
- 20% of the occurrences are unilateral meaning only one side of the vertebra is affected. Anatomically, there is a right and left pars interarticularis on each vertebra.
Sporting activities that involve a lot of low back extension and rotation correlate strongly with the occurrence of acute spodylolytic injuries. These include but are not limited to Lacrosse, Volleyball, Football, Baseball, and Gymnastics.
While spondylolysis is relatively common in adolescent athletes, there are substantial disagreements in the literature concerning the best methods for diagnosis and treatment, radiologic imaging, and the extent of activity restriction vs. the use of bracing. Many facilities advocate the routine use of a lumbosacral orthosis or brace in the management of these patients, with durations of its use ranging from a few weeks to a year. The braces range from soft corsets to rigid braces. Studies have shown that healing of bone takes place with the use of a rigid brace, a soft brace and no brace at all. The efficacy of bracing has not yet been revealed.
Establishing the diagnosis of spondylolysis requires that a pars lesion be identified with radiographic imaging. Neurological testing is typically expected to reveal normal results. A few orthopedic tests can prove to be positive, however they cannot definitively diagnose the condition. CT scans are currently the standard in the diagnosing of pars interruptions with plain film x-ray having a fairly limited role.
Rest is generally recommended for a period of 2-4 months following the diagnosis followed by a systematic rehabilitative strategy to reintroduce the sport to the athlete. In addition, due to the high incidence of hamstring tightness among athletes with this injury, a stretching regimen is added to the rehabilitation. This strategy includes low-impact cardiovascular training, early core stability training and a broad kinetic chain assessment. The athlete is gradually reintroduced to sport specific training and once range of motion is full with zero pain under sport specific stresses, the athlete is then granted a complete return to play.